ABDOMINAL AORTIC ANEURYSM SCREENING
vascular.co.nz>aneurysm screening
What is aortic aneurysm screening and why is it important?
Can screening programmes prevent aortic aneurysms?
When can a screening programme be successful?
What will happen if I agree to screening for aortic aneurysm?
What happens if the ultrasound finds an aortic aneurysm?
What is the evidence to support aortic aneurysm screening?
Is aortic aneurysm screening taking place in other countries?
Should women be screened for aortic aneurysm?
An example of how aortic aneurysm screening might work in Taranaki
What is aortic aneurysm screening and why is it important?
Abdominal aortic aneurysms (AAA) are dilatations of the major artery (aorta) within the abdomen. They are a potentially fatal condition because the artery can sometimes burst and if this happens most patients will not survive. Approximately 50-75% of patients with a ruptured aneurysm will die before they reach hospital. Of the survivors about one half will reach the operating theatre. Only about 40% of patients undergoing surgery will survive to 30 days. Most patients with a ruptured aortic aneurysm will not survive.
In contrast if an aortic aneurysm is discovered before it bursts the risk of dying from planned surgery for an AAA is around 5% (1 in 20). This is still an important risk, but much lower than that of a ruptured aneurysm. The vast majority of patients having planned aortic aneurysm treatment will survive.
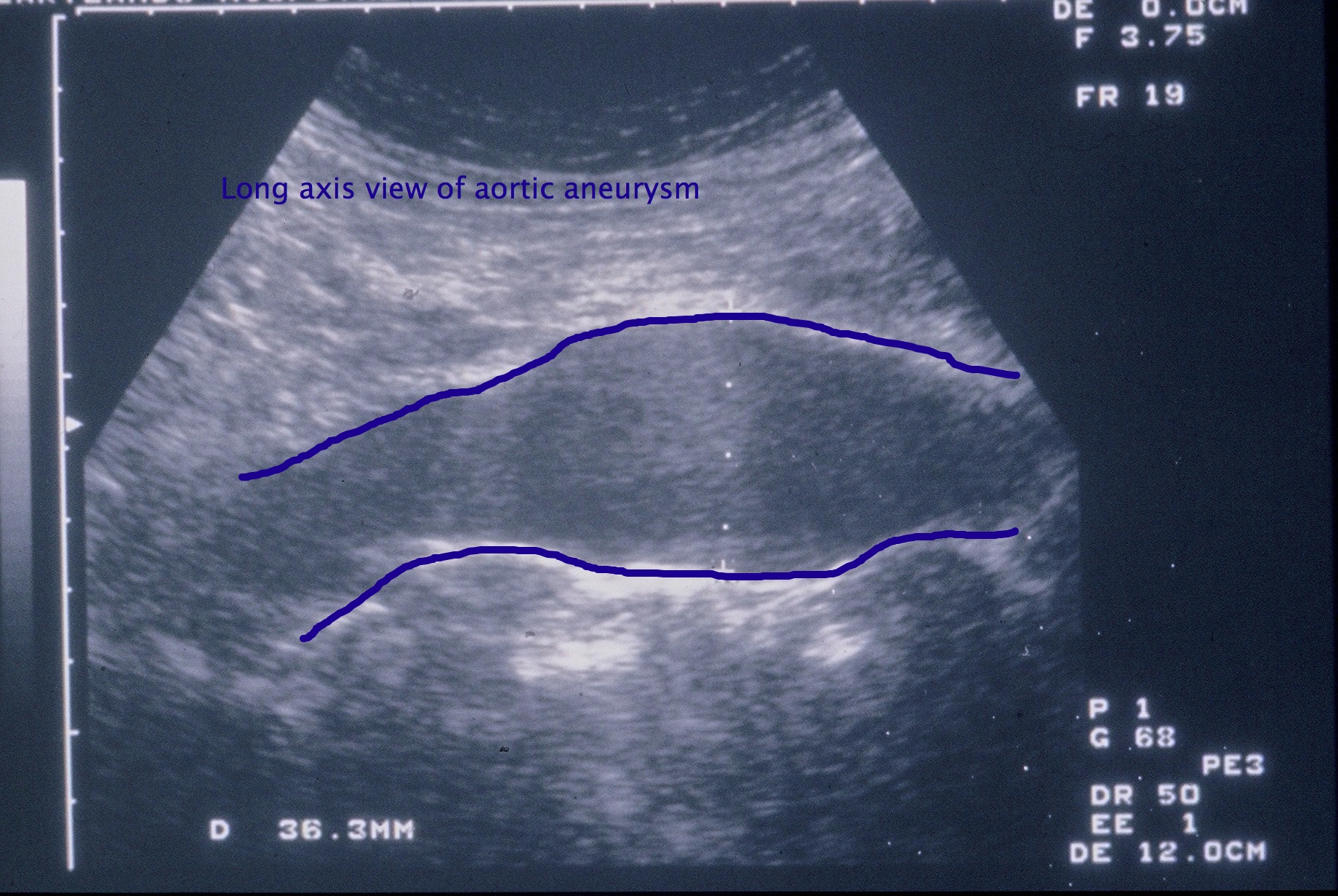
The risk of an aortic aneurysm bursting is related to its size, which is usually measured as the maximum diameter on an ultrasound scan (see below). The normal diameter of the aorta is approximately 20-25mm. Large aneurysms are more likely to rupture but two major studies have recently shown, that for small AAAs less than 55mm (or 5.5cms) in diameter, the risk of rupture is low at approximately 1% per year (1 in 100). Unfortunately, for most patients there are no symptoms that are caused by aortic aneurysms until they burst, so they are frequently not detected at a smaller diameter when they have much less risk of bursting.
As aneurysms can be a serious health issue much effort has been directed at trying to identify aneurysms when they are small and before they rupture. This is what an aneurysm screening programme will attempt to do. Screening programmes attempt to detect patients with aortic aneurysms when they are small and at low risk of rupture. They can then be monitored as they usually enlarge slowly over a period of years. Planned and safer treatment for the aortic aneurysm can then be arranged at an appropriate time
The development of a screening programe for AAAs which would detect aneurysms at an early stage (<5.5cms) when they are safe to monitor might avoid rupture in the majority of patients by giving these patients the opportunity of planned surgery to repair their aneurysm.
Can screening programmes prevent aortic aneurysms?
Screening programmes cannot prevent aortic aneurysms. They can only identify aortic aneurysms and then depending on their size a decision can be made as to the best management of the aneurysm. Screening programmes are able to minimise the chances of an aortic aneurysm rupturing by treating it at an early stage.
At present there is no known method of preventing aortic aneurysms. It may be possible to slow the expansion of aneurysms by treating standard vascular risk factors (see hardening of the arteries)
When can a screening programme be successful?
An effective screening programme for any disease has a number of requirements which are:
-
The disease should be an important health problem - AAAs account for approximately 400 deaths per year in New Zealand and the incidence of AAAs is increasing. It is a disease predominantly seen in men. A screening programme already exists for cervical cancer which claims the lives of approximately 60 New Zealand women per year.
-
The disease must have a high prevalence - AAAs are much more common in men and in certain high risk subgroups such as male first degree relatives of men with AAAs. AAAs increase in prevalence with age. AAAs are found in approximately 8% of men between 60 and 80years and are 6 times commoner in men than women.
-
The biological behaviour of the disease must be known - the natural history of AAAs is reasonably well understood. The rupture risk for AAAs less than 5.5cms (55mm) in diameter is approximately 1% per year. We now know from 2 major studies comparing early treatment with monitoring for small AAAs (<5.5cms) that it is safe to avoid operation until the aneurysm has expanded to 5.5cms unless it is rapidly expanding or becomes symptomatic.
-
The disease has a screening test which is sensitive, specific, safe, cheap and well tolerated - Ultrasound scanning is a sensitive, specific, quick, painless and completely safe investigation for the detection of AAAs. A single normal ultrasound scan (aortic diameter <26mm) at age 65 years will rule out significant aneurysm disease for life in men. Although clinical examination may detect an AAA, it is not very sensitive. In a study comparing ultrasound with clinical examination only 2 of 9 aneurysms found on imaging were detected by clinically experienced observers (Allen et al 1987).
-
Effective and acceptable treatment must be available - effective treatment is available in the form of operative repair either by an open or endovascular technique depending on the shape of the aneurysm.
- The screening programme must be cost effective - a large UK trial has calculated that it is cost effective to screen for AAAs in men and that the cost per year of life saved in the first 10 years was just £7,600 (approx NZ$17,500). The cost-effectiveness of aneurysm screening
is
comparable with other screening programmes (Thompson SG et al 2009) with a cost per life-year gained one third of the published cost per life year
gained with breast cancer screening or colorectal cancer screening and one
eighth the cost per life-year saved with cervical cancer screening.
What will happen if I agree to screening for aortic aneurysm?
At present in New Zealand there is no screening programme. If a screening programme were to be developed it might work as described below. You would be invited to attend for a free ultrasound scan if you were a man between the ages of 65 and 74 yrs old. An ultrasound scan is a scan commonly used to examine the baby during pregnancy. It is safe and painless and usually will only take a few minutes to determine whether an AAA is present. Examples of ultrasound scans are shown in the black, white and blue images. Patients with a normal scan will not usually need any further follow up.
What happens if the ultrasound finds an aortic aneurysm?
If an aortic aneurysm is identified, the next step will depend on the size of the aneurysm. Patients with AAAs less than 4cms in diameter would require scans at 2-5 year intervals. For aneurysms from 4-4.4cms scans would be annually. For aneurysms of 4.5-4.9cms scans would be at at 3-6 monthly intervals. For AAAs 5-5.4cms scans at 3 monthly intervals are needed. Some authorities advocate 3 monthly scans once the aneurysm reaches 4.5cms. Once an aneurysm has reached 5.5cms consideration should be given to treating the aneurysm and this will be appropriate in most patients. In some patients with other conditions that make treatment more hazardous it may be appropriate to wait until the aneurysm has enlarged further. This is because it is always important to balance the risk of treatment against the risk of rupture of the aneurysm. Although the risk of rupture may be slightly greater if an aneurysm is left until it is larger it may still be safer than the surgical risk.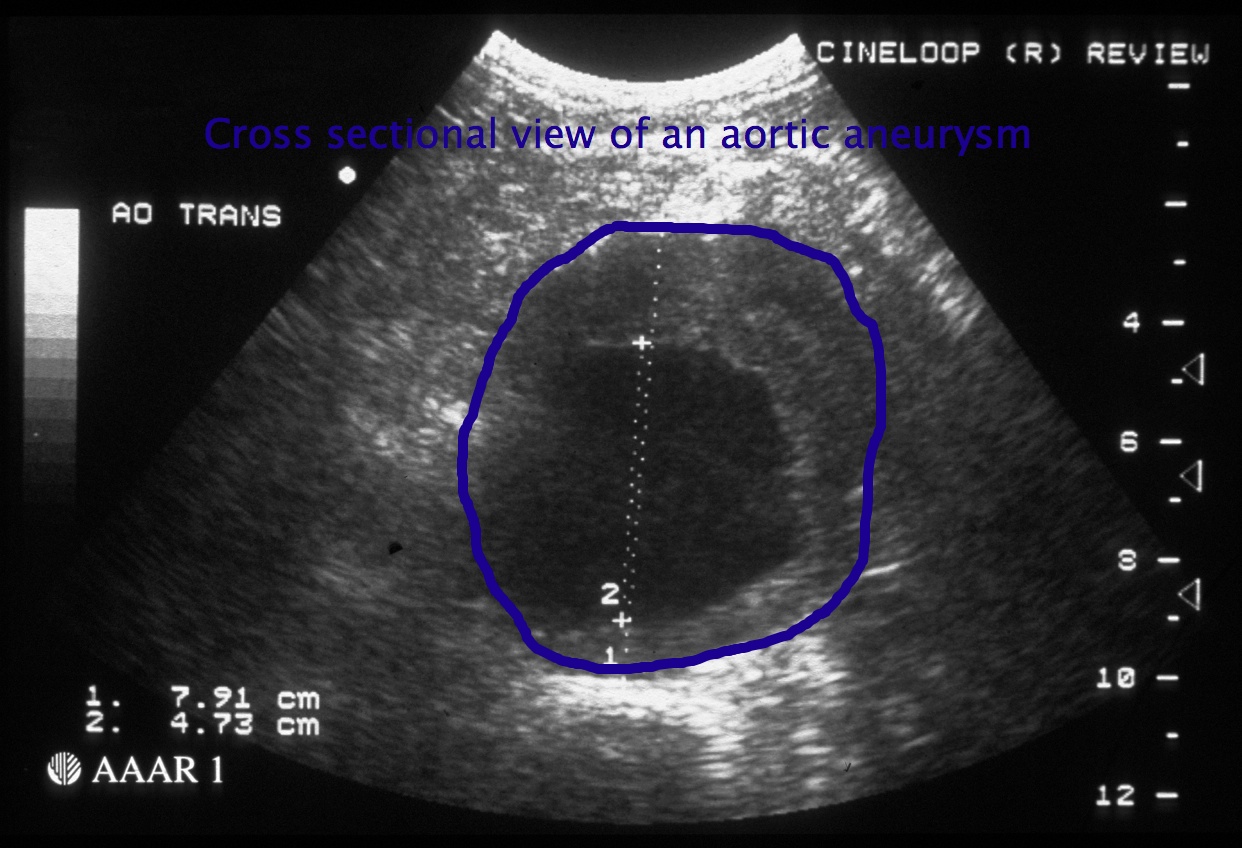
Patients whose AAAs are less than 5.5cms would not be offered treatment unless the AAA was rapidly expanding at more than 1 cm per year or became symptomatic. This is because at the smaller size it is as safe to monitor aneurysms as it is to repair them surgically. It is impossible to prevent all ruptures but screening will reduce this to a minimum. We also know that for small aneurysms that are regularly monitored approximately 60% of patients will eventually need surgery.
What is the evidence to support aortic aneurysm screening?
The Multicentre Aneurysm Screening Study (MASS) funded by the UK Medical Research Council recuited 67,770 men aged 65-74 years and randomised them to ultrasound screening for aneurysm or no screening. Of the men who attended for an ultrasound 4.9% had an AAA more than 3cms (1334 aneurysms in 33883 screened). After 10 years of follow-up there was a 48% relative risk reduction in the risk of death from aneurysm rupture in the patients screened with an ultrasound scan (absolute risk reduction 0.87% to 0.41%). An editorial in the British Journal of Surgery called for the widespread introduction of aneurysm screening in the UK and a national UK programme is currently being rolled out.
Is aortic aneurysm screening taking place in other countries?
In the UK the national screening body is gradually rolling out screening across England. All men will be invited for screening when they turn 65 years old. The image below is a screenshot of the UK NHS screening website. There are no other nationally funded screening programmes for aortic aneurysm. There is also a detailed leaflet for GPs with information on how screening is to take place in the UK and how follow-up will take place.
Should women be screened for aortic aneurysm?
Screening studies target men because aortic aneurysms affect men much more commonly. There is some evidence that screening for women may also be cost effective because of their longer life expectancy and increased risk of rupture (Wahhainen A, 2006). Aneurysms in women, when they do occur, seem to enlarge slightly faster than in men (Mofidi R et al, 2007). At present because of the lower rate of aneurysms in women there are no proposals for screening programmes.
An example of how aortic aneurysm screening might work in Taranaki
Age Grp |
Maori | Non-Maori | Total |
65-69 |
120 |
1875 |
1995 |
70-74 |
69 |
1716 |
1785 |
To give an example of what could be achieved with a screening programme I have worked out approximate screening numbers for Taranaki based on 2001 census data. In men 65-74yrs old the programme would screen approximately 3780 men. Approximately 148 (4.9%) aneurysms in 3024 men would be identified assuming 80% of men accepted the invitation to be screened. In 105 (71%) of these AAAs the diameter would be between 3-4.4cms. Twenty five (17%) would be medium size AAAs (4.5-5.4cms) and 18 (12%) would be large aneurysms (5.5cms or greater).
Recent Press release 13th June re abdominal aortic aneurysms
References
The UK Small Aneurysm Trial Participants. Mortality results for randomised controlled trial of early elective surgery or ultrasonographic surveillance for small abdominal aortic aneurysms. Lancet 1998; 352: 1649-1655.
Lederle FA, Wilson SE, Johnson GR et al. Immediate repair compared with surveillance of small abdominal aortic aneurysms. New Engl J Med 2002; 346: 1437-1444.
Cheatle TR. The case against a national screening programme for aortic aneurysms. Ann R Coll Surg Engl. 1997; 79: 90-95.
Boll APM, Verbeek ALM, Van de Lisdonk EH, Van der Vliet JA. High prevalence of abdominal aortic aneurysm in a primary care screening programme. Brit J Surg 1998; 85: 1090-1094.
Allen PIM, Gourevitch D, McKinley J, Tudway D, Goldman M. Population screening for aortic aneurysms. Lancet 1987; 736.
Crow P, Shaw E, Earnshaw JJ, Poskitt KR, Whyman MR, Heather BP. A single normal ultrasonographic scan at age 65 years rules out significant aneurysm disease for life in men. Brit J Surg 2001; 88: 941-944.
Bengtsson H, Norrgard O, Angquist KA, Ekberg O, Oberg L, Bergqvist D. Ultrasonographic screening of the abdominal aorta among siblings of patients with abdominal aortic aneurysms. Br J Surg 1989; 76: 589-591.
The Multicentre
Aneurysm Screening Study Group (MASS) into the effect of abdominal aortic
aneurysm screening on mortality in men: a randomised controlled trial. Lancet
2002; 360: 1531-1539.
Beard JD. Screening for abdominal aortic aneurysm. Brit J Surg 2003; 90:
515-516.
Thompson SG et al Screening men for abdominal aortic aneurysm: 10 year mortality and cost effectiveness results from the randomised Multicentre Aneurysm Screening Study. Brit Med J 2009; 338: 1538-1541.
Wanhainen A,
Lundkvist J, Bergqvist D, Bjorck M. Cost-effectiveness of screening women
for abdominal aortic aneurysm. J Vasc Surg 2006; 43: 908-914.
Mofidi R, Goldie VJ, Kelman J et
al. Influence of sex on expansion rate of abdominal aortic aneurysms.
Brit J Surg 2007; 94: 310-314.
Last updated> 21 August, 2010
![]() Bookmark this on Delicious
Bookmark this on Delicious  reddit
reddit 
![]() facebook
facebook